

Discovering My Gender-Bendy Prenatal History
Various hormone-disrupting drugs, used in abundance in millions of pregnancies over many decades, may be quietly distorting human development.


Reality’s Last Stand is a reader-supported publication. Please consider becoming a paying subscriber or making a one-time or recurring donation to show your support.

About the Author
Jill Escher is an autism research advocate and philanthropist based in the San Francisco Bay Area. Learn more at jillescher.com.
In 1973, when I was eight years old, a stranger began making regular visits to my family’s home in Los Angeles. She would seat me at my father’s desk, administer some tests, watch me as I played, and ask questions such as, “Do you like to play with dolls?” After each session I would receive a crisp $5 bill, which made me feel oh-so-important. When I asked my mom what these visits were about, she simply said, “To find out just how smart you are.”
Perhaps that’s what she thought, but she was wrong. In the early 2010s, through a chain of small miracles, I unexpectedly discovered the true purpose of those encounters. It started with a vague wisp of a memory of my father once calling me “a miracle child.” This memory sparked a curiosity about potential 1960s fertility treatments, leading me to ask my mom about it. She responded enthusiastically, “Yes, I was so lucky, Dr. Tyler was fabulous! And he also wrote jokes for Groucho Marx!” Encouraged, I obtained my mom’s 1965 obstetric records from when she was pregnant with me, thanks to her and her unusually meticulous OB's office that had preserved them on microfiche. During my research, I stumbled upon a curious term scrawled in the records that was hard to decipher. After several attempts, I typed “Deluteval” into Google.
This search coughed up a 1977 paper from the journal Archives of Sexual Behavior titled “Prenatal exposure to synthetic progestins and estrogens: Effects on human development,” authored by June Reinisch and William Karow. The abstract explained that the retrospective study assessed IQ and personality outcomes in 71 offspring of “mothers administered combinations of synthetic progestins and estrogen for the maintenance of at-risk pregnancy.”
I Was Exposed To … What?
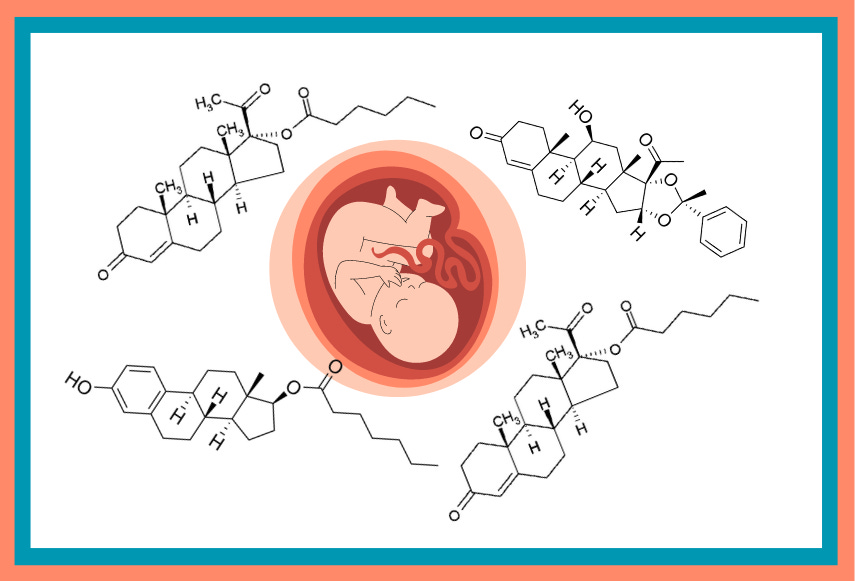
As I read, I felt the world changing colors and my jaw dropped to the floor. Using names and terms from my mom’s old medical files, combined with my memories of home visits from my childhood, I instantly realized that I was one of those 71 exposed children. Reading further, I saw that Deluteval was the brand name of one of 37 different hormone drugs administered in various mixes, doses, and durations to these pregnant women (see Figure 1).
At last, a thin layer of fog lifted: for some reason, my mother had been prescribed a regimen of synthetic sex hormones during her pregnancy with me because, at the time, it was (falsely) believed that these drugs could prevent miscarriage or mitigate other pregnancy risks. But what specific sex hormones was my mother given? And to what effect?

This was hardly a trivial question. I was acutely aware of the catastrophe of the fake estrogen drug, diethylstilbestrol (DES), which was administered to more than 10 million pregnant women worldwide from the baby boom era through 1971, and even later in many cases. This lab-made pseudo-hormone had been widely hyped as an anti-miscarriage treatment or a sort of vitamin that helped produced larger, healthier babies. It was even more heavily used in the livestock industry, causing additional low-level human exposure until it was phased out in 1979.
However, instead of producing healthy babies, DES was a teratogenic chemical mutilator later found to increase risk for a laundry list of horrors for the exposed offspring. In females, these included but were hardly limited to, vaginal and cervical cancer, breast cancer, malformed uterus and fallopian tubes, infertility, and miscarriage. In males, it was linked to testicular cancers, penile and testicular abnormalities, and gender identity differences.[1]
DES provided a nightmarish lesson of what can go awry when we tamper with nature’s hormonal blueprint—a set of precise molecular instructions for fetal development that has evolved over hundreds of millions of years. Indeed, the disaster was fresh in my mind because, shortly before stumbling on the Reinisch paper, my dear friend Erin’s older sister Mary, a victim of DES exposure who battled infertility and aggressive breast cancer, tragically died at age 59. These hormones were more than just odd multisyllabic drug names on a page; they could also be deadly poisons.
Although I could not determine the nature or extent of my own exposures, I noticed that those of us exposed to progestins (synthetic molecules with progesterone-like effects) and smaller amounts of synthetic estrogens, including DES, had exhibited shifts in personality. We were often described as more independent, sensitive, self-assured, individualistic, and self-sufficient, yet less cortically alert. Those exposed to higher doses of estrogens were more group-oriented, and less independent or self-assured.
The report also detailed the earlier research finding that synthetic sex hormone drugs could masculinize or defeminize females, or demasculinize or feminize males, both in terms of body and behavior. It also highlighted the absence of evidence that these drugs actually reduced the risk for miscarriage or other complications. Furthermore, it revealed that the mothers often had minimal knowledge or recollection of the drugs they were administered, even when injected with synthetic sex hormones twice a week. This certainly applied to my mother, who only remembered being given “lots of stuff.” The study immersed me into a dark and mysterious medical past, leaving my head spinning.
Calling Dr. June
To learn more, I sought to contact the study’s lead author, Dr. Reinisch,[2] hoping she was still alive. I was gratified to locate the spirited and Brooklyn-accented “Dr. June,” who had become a renowned researcher and director of the Kinsey Institute, the Indiana-based center for sex research, although she was now mostly retired. She confirmed that I was very likely one of her study subjects, although it was a research assistant, not she, who had made those visits in 1973. She offered to send me the files about my exposures. “We have safe-guarded all the records from our studies,” she wrote. “They are locked in the confidential files of The Kinsey Institute.”
It was a rather strange feeling to discover, after more than 45 years of a fairly humdrum life, that a center for sex research kept secret files about my sex hormone exposures. However, by this point, the revelation felt like just another surreal detour on a treasure hunt concocted by the ghost of Rachel Carson. Eventually, Kinsey staff located the files about my mother’s treatments and sent them to me, with Dr. June remarking that I might be a bit shocked by what I’d find.

“Heavily treated” was written at the top of one file, and the OB records combined with the research records including the fertility specialist’s additional treatments indicated that my mother had undergone a progestin-heavy regimen:
For the first trimester:
Deladroxate (dihydroxyprogesterone acetophenide, about 100 mg, combined with 10 mg estradiol enanthate [Squibb]), administered via weekly injections for 7 weeks, totaling 700 mg of the progestin and 70 mg of the estrogen.
Prednisolone (also indicated as “Sterane” [Pfizer]), orally, approximately 35 mg per week for 10 weeks.
For the second and third trimesters:
Deluteval 2X (hydroxyprogesterone caproate 250 mg, combined with 10 mg estradiol valerate [Squibb]) given by weekly injection for 19 weeks. This results in about 4,750 mg of progestin and 190 mg of estrogen. A hole punch in the file made the first digit of a relevant notation illegible, but these figures align with what was standard practice according to the literature at the time.
In total, my mother was given approximately 5,500 mg of synthetic progestins and about 260 mg of synthetic estrogens, not to mention the months of prednisolone, a corticosteroid. To provide some perspective, while the chemical structures and compositions of contraceptive drugs are now different, a birth control pill today typically contains 1 mg of synthetic progestin and 10 mcg of synthetic estrogen.
Dr. June explained to me the enormity of the post-war mad-scientist approach to excessively medicating pregnant women, when the field glorified excessive doses of the new “miracle drugs,” despite lacking research demonstrating their efficacy or their effect on fetuses. The prevailing myth at the time was that a placental barrier protected the baby from harm, which led to minimal testing for adverse effects by pharmaceutical companies. “Medical practice was based on theory, not evidence,” she told me, noting that doctors often prescribed whatever drug representatives happened to bring by that month. In truth, we kids were unwitting guinea pigs in a vast human medical experiment.[3]
It was a common medical practice to preemptively drug pregnant women for a number of reasons: previous miscarriage, advanced maternal age, prior preterm birth, prior stillbirth, multigravida (i.e., twins), spotting, chronic conditions like diabetes, and other issues. My mother was referred to a fertility specialist after suffering two miscarriages—a history that, although not unusual, once labeled women as “habitual aborters” and targeted them for intense “pregnancy maintenance” therapies.
Exposure to these drugs were not spread evenly throughout the population. A large U.S. study, the Collaborative Perinatal Project, which involving tens of thousands of pregnancies at public hospitals, found that 5 percent of pregnancies in the late 1950s and early to mid-1960s received such treatments. However, rates were much higher in private clinics and hospitals, like the clinic where my mother was treated, where wealthier women could afford these drugs.
With her team, Dr. June conducted numerous research studies across two continents and several decades on the impacts of synthetic hormones. She generally concluded that, apart from teratogenic impacts in some cases, the drugs had the effect of “flavoring” us. The temperament and personality “flavors” she observed in the exposed children were “red flags,” indicating that the hormones caused physiological changes in the children’s brains. This was to be expected with the introduction of huge doses of foreign, exogenous hormones. These hormone imposters interfered with the natural signaling involved in developing typical male and female brains. In the case of my high-dose progestin group, she noted that we (females) developed “a more masculine configuration.”
“A More Masculine Configuration”: The Awesome Power of Sex Hormones
Biochemically, this made perfect sense to Dr. June. Synthetic sex hormones can hyper-activate, prolong, or block normal gene expression and activate receptors intended for other hormones. They can produce unpredictable and cross-sex effects.
It’s impossible to overstate the fundamental role of sex steroids in shaping human development. While people focus on XX and XY chromosomes, their role, while absolutely pivotal, is somewhat time-limited. A specific site on the Y chromosome prompts the embryonic proto-gonad to develop into testes. But once the male or female gonads take shape as part of a larger endocrine system, their hormones—mainly estrogen and progesterone in females, and mainly testosterone in males[4]—take control of sexual differentiation of the brain and body.
The reason sex steroid hormones have an effect, however, is due to the steroid hormone receptors—countless proteins populating cells in a wide variety of tissues, from bones to muscles to reproductive organs and brains. The hormones first bind to their nuclear receptors, like a key in a lock. Then together they act as transcription factors, a complex that binds to the promoter region of their target genes, thereby triggering gene expression along a hormone-specific developmental cascade.[5]
Defects in hormonal signaling—whether innate or externally imposed—can lead to deviations from normal sexual differentiation of the brain, body, or both.
Case in point 1, faulty androgen receptors: Androgen insensitivity syndrome (AIS) is a rare genetic disorder in which an XY male with testosterone-releasing gonads (testes) develops along a female or even hyper-feminine pattern. This occurs because the affected person’s body tissues lack functioning androgen receptors and thus cannot respond to testosterone. This results in the default to female-like gene expression. Even XX females have some testosterone that binds with their androgen receptors, meaning that XY AIS individuals can exhibit even more pronounced feminization than XX females. For a good example of AIS in a highly feminine XY individual, please watch Sara from Finland in this video in which she comes out as intersex.
Case in point 2, virilized girls: The earlier generation of synthetic progestins, used before those given to my mother, had stronger androgenic effects, often causing physical virilization in exposed girls. Severe birth defects included micro-penis-like enlarged clitorises, scrotum-like fused labia, and a conjoined urethra and vagina, known as a urogenital sinus. Unlike natural progesterone, synthetic progestins can interact with androgen receptors, triggering a masculinizing developmental cascade in females.[6]
Case in point 3, estrogenized boys: If a male embryo/fetus experiences low or no exogenous estrogen exposure during the first several months, he is likely to develop a normal male reproductive system. However, if he is whomped with a potent estrogenic drug like DES during mid to late gestation—a critical period of brain development—his brain may develop along a more female-typical pattern. While it’s impossible to have a brain of the opposite sex to your body, the effects of DES can produce cross-sex brain patterns.[7]
Let me share stories about two biological men with feminized brains.[8] I recently spoke with a man I met though a DES support group. Born in 1958 in Texas, he spent all his life despairing over his lack of masculine behaviors despite having male anatomy. Though married with two grown children, he now somewhat identifies as a woman and has started estrogen therapy, which has brought him tremendous psychological relief. However, his lifelong struggle with a felt dissonance between his brain and body—an internal ache not entirely imposed by society—was a circle of hell even Dante would be hard-pressed to dream up.
Consider also the plight of another DES son, later named Rhondalynn Chocolatehaus, who was part of our online group and clearly born with a DES-feminized brain in a male body. He (who later adopted “she” pronouns) was born in 1961 in Massachusetts with ambiguous genitalia (an indicator that his mother took DES very early in pregnancy) and was subjected to childhood genital surgery to appear more male. Raised as a male, he later transitioned in his mid-40s and underwent sex reassignment surgery, which led to chronic pain. Suffering from severe depression and threats from the religious right in the North Carolina community, Rhondalynn committed suicide in 2016. Her brother, also a DES son, had already committed suicide.[9]
Additionally, consider that even without a toxic exposure like DES, natural endogenous processes can lead to a non gender-conforming orientation. For instance, research suggests that some women who have successive male children may produce an antibody that increases the likelihood that males later in the birth order will be gay.
Despite not being trans or gay myself, I felt Dr. June’s “more masculine configuration” remark quite deeply. Though boy-crazy and firmly heterosexual from the start, I was always helplessly tomboyish—a trait described by my late friend Feda Almaliti as “so androgynous.” It’s not like I wanted to be; I struggled to act more girlish and feminine, but it was a lost cause. Clothes with frills or flowers or flounces or lace or anything girlie made me miserable. Despite desperately wanting to, I couldn’t bring myself to grow my short hair past my ears.
Peering Into a Hidden History
Now, if I was a tad gender-bent by exposure to synthetic sex hormones, what of the tens of millions of people who, unbeknownst to them, had suffered similar exposures, albeit perhaps with different mixtures, doses and timings? Dr. June called it a vast “hidden history,” and she worried about the long-term individual and population-wide consequences of evolutionarily unprecedented pregnancy drugs.
Though the use of synthetic estrogens waned in the 1970s, progestin-based protocols remained in widespread use for decades until just last year. In 2023, the FDA finally revoked approval for the last of these drugs, marketed as Makena (technically 17-OHPC, the same progestin in Deluteval and Delalutin). This decision followed clinical trials showing it was ineffective. In May 2024, the European Medicines Agency recommended suspending the marketing authorizations for medicines containing 17-OHPC.
Makena is a poster child for scandalous pharma-bro excesses, with the drugmaker charging insurers $800 to $1,500 per shot—despite being ineffective and painful. As a compounded drug, the cost was about $15 per injection, so please marvel at this spectacular profit margin. To learn more about the Makena debacle, I highly recommend this presentation called “Beneficial to Whom? A Review of Makena and the FDA’s Accelerated Approval Process,” featuring two brilliant physicians, Dr. Ealena Callendar and Dr. Adam Urato:
Despite the widespread exposure of individuals to synthetic sex hormones and other hormone-disrupting drugs, knowledge and awareness of their potential fetal impacts has yet to seep into public consciousness. Apart from a few individuals, like some DES daughters whose mothers’ physicians disclosed their medical files after the drug’s cancer-causing properties were revealed, almost no one has access to their prenatal records. It was only through a series of ultra-rare flukes that I had any inkling about them, let alone detailed information about the aggressive treatments my mother received.
Unless drugs cause obvious birth defects—think of the thalidomide disaster of the late 1950s and early 60s that resulted in tens of thousands of babies being born with heartbreaking deformities such as limbless torsos—they seldom make headlines. Even widely used anti-seizure medications, known to cause physical and mental impairments in exposed offspring, are barely known for these effects. If there’s one thing I’ve learned through this whole ordeal it’s that countless millions of you are walking around oblivious to the (sometimes massive amounts of) drugs you were exposed to in utero. Almost all of your records are long gone, and you will likely never know their impact on your development.
It’s Time To Expand the Discourse
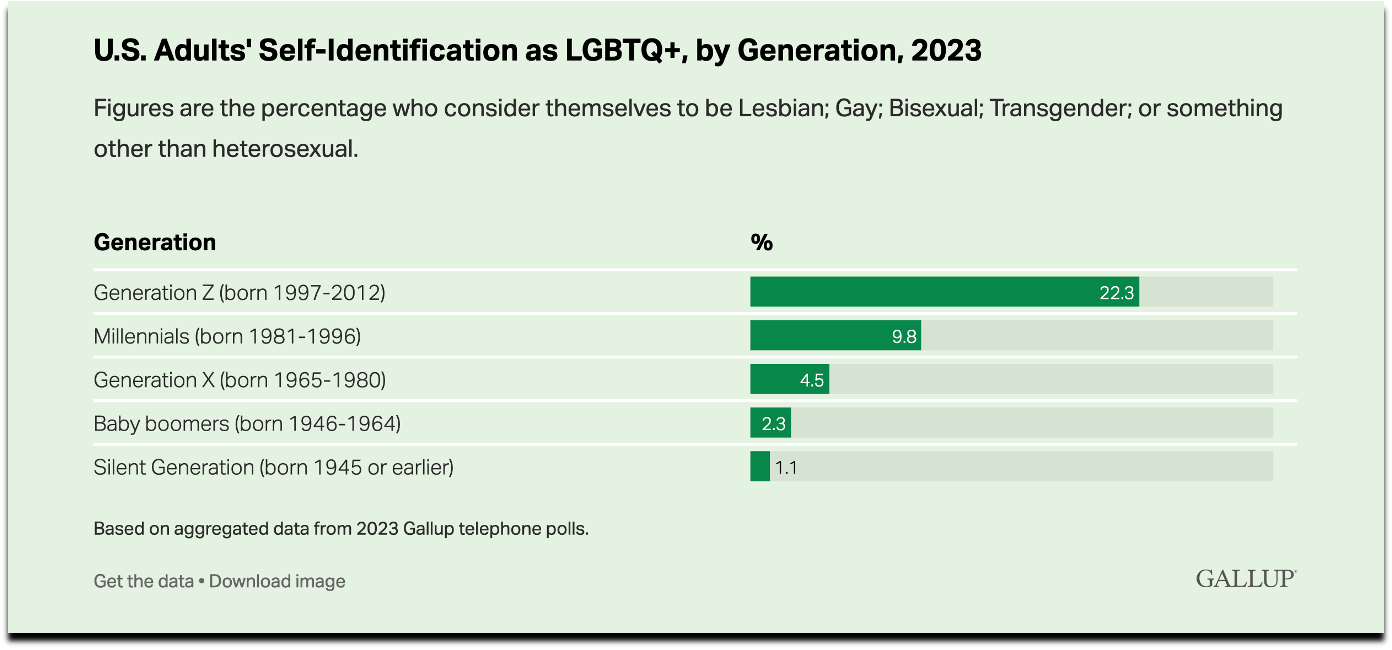
Recent decades have seen a dramatic 20-fold increase in LGBTQIA+ identities (Figure 3).[10] It seems that narratives about this phenomenon are divided into two camps. One side argues that the escalating rates of gender non-conformity simply reflect greater acceptance of always-existing but previously repressed sexual identities and forms of expression. The other side is concerned that social constructs and contagions might be unduly persuading young people to adopt new gender identities and undergo medical procedures that they may later regret and can cause lasting harm.
However, this debate strikes me as a bit naive, a bit too ideological, and a bit too lacking in context. Neither side seems to contemplate how this surge might in part be the outcome of a long history of drugs subtly reshaping, or at least re-“flavoring,” segments of humanity. The debate should not be limited to “it’s Pride” or “it’s TikTok.” There is also toxicology to consider.
Recent studies should raise our concern about progestins. For example, a 2016 study in animal models showed that early exposure to 17-OHPC impaired cognitive flexibility with increased perseveration later in life, particularly in males. A 2024 study found that early exposure to 17-OHCP resulted in impaired decision-making in adult female rats. Another study from 2021, more directly related to gender identity, found that 17-OHPC treatment reduced normal sex differences in cortical maturation.[11]
In humans, precious little research has been done, which should shock the conscience considering the widespread fetal exposure to these drugs. A 2007 study on 17-OHPC looked at potential impacts on gender-specific roles in exposed offspring, but the mean age at follow-up was just 4 years old, and the study did not include pubertal or reproductive development or other long-term safety questions. The authors also noted that the study lacked the ability to detect subtle changes. However, a 1980 study reported that young men exposed to 17-OHPC as fetuses recalled their boyhood behavior as more “feminine.” Additionally, a 1984 study found that adolescent males exposed to 17-OHPC in utero spent more time sedentary watching television than the control group, perhaps suggesting less time engaged in more active boyish pursuits.[12]
It’s also worth noting that a 2017 study by Dr. June herself on natural progesterone supplementation (another common anti-preterm birth strategy, but not 17-OHPC) found that fewer exposed males and females identified as heterosexual. More of them reported histories of same-sex sexual behavior, attraction to the same or both sexes, and scored higher on attraction to males. Exposure was associated with higher rates of bisexuality.
To my mind, the literature taken as a whole, although not as extensive as one might expect for such a common toxicant exposure, shows that progestins and unnaturally high doses of progesterone can alter socio-sexual development in exposed fetuses, adding to the tragic DES evidence and confirming Dr. June’s “flavoring” observations.
More importantly, we should consider other common medications that impact hormone signaling and also affect sexual differentiation of the brain. It’s not only synthetic sex hormones that alter how sex hormones work. This also includes anti-depressants, anti-psychotics, anti-epileptic drugs, general anesthesia, and medications used in IVF and assisted reproduction. Add to that a whole soup of endocrine-disrupting chemicals in our environment. To some extent, we are all still guinea pigs.
I don’t pretend to have all the answers. However, I do know we must be raising these questions.[13] We should all be concerned that my experience of being subtly masculinized by synthetic hormones might just be the small tip of a vast iceberg.
[Copyright 2024 Jill Escher]
Reality’s Last Stand is a reader-supported publication. If you enjoyed this article, please consider upgrading to a paid subscription or making a recurring or one-time donation below. Your support is greatly appreciated.
If you enjoyed this article, you may also like…




Notes
[1] Dr. Rachel Levine strikes me as possibly a classic case of prenatal DES exposure. While to my knowledge Dr. Levine, who at one point fathered children but now identifies as female, has never mentioned any DES exposure, that hardly precludes this possibility as it seems most DES sons do not know of their exposures (the 1971 vaginal cancer revelation which prompted some limited awareness related only to female offspring). The Boston area where Levine was born in 1957 was a hotspot for DES use, related to the fact that DES’s strongest advocates, Smith & Smith, were Boston-based and associated with Harvard. Because there is no biomarker for DES exposure the truth is pretty much out of our reach.
[2] To be clear, when I contacted Dr. June my primary, though not unitary, interest was in my eggs, not in my own brain or behavior, as I had two children with idiopathic severe autism, and had a hunch this highly abnormal and unexplained outcome in my offspring had something to do with perturbed epigenetic re-programming of my gametes. I first wrote about this in 2018 for the journal Environmental Epigenetics, and have continued to advocate for research on this question, including in the Journal of Autism and Developmental Disorders, Biology of Reproduction, and Environmental and Molecular Mutagenesis, as well as at many scientific conferences. My husband and I also fund pilot research grants looking at these questions of toxicant-induced non-genetic inheritance in autism and related disorders.
[3] Another paper on this study likening us exposed children to “experimental animals” with skewed personalities was published in 1977 in the crème de la crème scientific journal Nature. https://www.nature.com/articles/266561a0. For those who wish to dig deeper, please see my 2016 interview with Dr. June http://www.germlineexposures.org/reinisch-qa.html.
[4] All steroid hormones are structurally similar, but even minor differences (even estrogen and testosterone are not so structurally different) can profoundly alter biochemical activity.
{kind=link}
[5] A political tangent. People who know about my advocacy work in the field of sex hormones have asked about the hot topic of transgender women in sports. Sports by definition is about physical prowess. Biological men, even if they have been flavored by some degree of mental feminization, are still biological men, with countless physical advantages wrought by stages of developmental testosterone exposure. It’s not a tough question —it seems patently unfair for biological men who have had testosterone-based growth to compete in women’s sports, no matter how gender-diverse their brains my feel.
[6] Another political tangent. Given this tragic history, what about testosterone use by male-identifying biological females who become pregnant? Testosterone is a teratogen that would strongly raise the risk for virilizing a female fetus. By any moral standard, biological females who are transgender men planning to get pregnant should take the greatest care to avoid testosterone exposure from periconception through lactation (if any). Unbelievably, some trans advocates in true Twilight Zone fashion have contended that preventing such birth defects amounts to “eugenics.”
[7] Please consider that the same hormone drugs intentionally used to induce feminization (e.g., Deluteval) or to chemically castrate males (e.g., DES) were used routinely as pregnancy drugs, for decades. Most notoriously, DES was used to chemically castrate the genius Alan Turing in early 1950s.
[8] A 2024 French study found sharply increased transgenderism in biological males who had been fetally exposed to DES. https://www.mdpi.com/2039-4713/14/1/10
[9] A groupmate said of Rhonda, a master chocolatier: “One time she messaged me and asked me if I could secretly get someone's address so that she could surprise them with some of her chocolates because she thought they needed some cheering up. That is the kind of person she was. She had so much talent and so much to offer. Twice she tried to buy buildings to open shop but when the owners discovered she was transgender they backed out of the deals.” In her final message before killing herself she asked our community to “keep the fight going” and even before then was public with her story, which is why I feel comfortable, even compelled, to share it here.
[10] Recent decades have seen sharp increases in ADHD, autism, anxiety, depression, urogenital defects such as cryptorchidism and hypospadias, infertility and declining sperm count, and even some forms of cancer. I would submit that all these phenomena are likely inter-related to some extent and have at least some roots in direct or generational effects of toxicant exposures.
[11] Worryingly, a 2022 epidemiological study on prenatal 17-OHPC found long-term risks for offspring cancers. Exposure in the first trimester was associated with an increased risk of any cancer, and the risk increased with the number of injections. Exposure in the second or third trimester conferred an additional risk for the male but not for the female offspring. The risk of colorectal, prostate, and pediatric brain cancer was higher in the offspring first exposed to 17-OHPC in the first trimester.
[12] A 2018 study from China found an association with prenatal progestin exposure and autism risk.
[13] Of greater concern may be impact on the parental germ cells (egg, sperm and their precursors) which in turn influence offspring outcomes, and may help explain the increases in a number of heritable disorders, including autism.
 | A guest post by
|
Thank you for this very thought-provoking article. You are correct in that there is a complex relationship between societal/environmental factors and biology (from molecules to systems) that, together, shape the person that we become. It is also true that the interactions are complex and often poorly understood even by the so-called experts. Https://everythingisbiology.substack.com/p/there-is-biological-evidence-for
Thank you again for this very interesting read. Sincerely, Frederick
What a great and well researched piece, thanks for your efforts to write this.
Besides providing some really interesting data and scientific discussion, I was struck by your comment that it's time to expand the discourse (especially struck by being able to get this posted on this particular Substack!). Unfortunate that the current discourse is being so ideologically driven right now, rather than focusing on the biological complexities you consider in the context of humanity.