

Jack Turban’s Research Is Incapable of Answering the Questions It Attempts To Address
Jack Turban’s papers are peer ‘affirmed’ instead of peer ‘reviewed.’



Reality's Last Stand is a reader-supported publication. All articles are free, but if you would pay to access this article behind a paywall, please consider becoming a paying subscriber anyway, or making a one-time or recurring donation. I’d rather a million people view this content for free than have it be accessible to only a small group of paying subscribers, but that means I rely fully on the generosity of my readers for support. Thank you!

In the ongoing scientific debate regarding transgender identification among children and adolescents—and the corresponding debate about how medical and psychological services can best meet the needs of these young people—a major point of contention is over what’s referred to as “gender affirming care.” This model of care directs clinicians to avoid questioning a minor’s self-declared gender identity and desire to medically transition, which often includes puberty blockers, cross-sex hormones, and surgeries.
One of the leading proponents of this controversial protocol is Dr. Jack Turban, a researcher whose work is frequently published in popular mainstream media outlets as well as high-impact medical journals. Although his articles receive glowing praise among gender activists and clinicians who are strongly biased in favor of gender affirmation, his work is widely viewed as over-sold, sloppy, and highly misleading by his critics.
A recent paper of Turban’s was published in the journal Pediatrics that purported to debunk the notion that the dramatic rise in youth referrals to gender clinics for gender dysphoria is due, in part, to “social contagion.” More specifically, Turban et al. claim to have examined and failed to find support for two hypotheses: (1) that youth identify as trans due to social contagion, with female adolescents being more susceptible; and (2) that youth identify as trans to flee LGB-related stigma.
This study drew sharp criticism not only from the usual critics of gender affirmation, but also from die-hard proponents of gender affirmation concerned that Turban’s flawed methods would only provide fuel for the other side. While much has already been said about Turban’s Pediatrics paper, I will add to the chorus of criticism by addressing whether the study’s design, data, or methods stood any chance of ever supporting the hypotheses it set out to evaluate.

Perhaps smarting from past criticism pointing out that most of his work mines the very non-random U.S. Transgender Survey, Turban has turned his attention to the Youth Behavioral Risk Surveillance System (YRBSS) survey administered by the Centers for Disease Control and Prevention (CDC). This is indeed a much more representative dataset, and for questions administered across the United States, one can employ the included survey weights to generate nationally representative statistics. The survey itself uses a complex survey design, meaning that individual geographic areas are selected randomly, but then individual student responses are clustered. This is because the survey is administered in schools, and it is not practical for it to be entirely random. Sampling weights, including variables indicating how the data are clustered, are included for the exact purpose of correcting for these issues.
Turban and other proponents of physical and medical interventions for gender dysphoric youth have spent significant energy over the past few years attempting to discredit the work of Dr. Lisa Littman, the independent academic researcher whose 2018 paper first documented the appearance of a new cohort of individuals presenting with gender dysphoria. She coined the term “rapid-onset gender dysphoria” (ROGD) to describe a set of circumstances reported by parents participating in her study: adolescents who announced a transgender identity at or shortly after puberty after no childhood history of gender dysphoria. Parents reported that their teens, 83 percent of whom were female, had numerous co-occurring mental health issues, autism spectrum diagnoses, were disproportionately gifted, and appeared to have gravitated to transgender identities after extended periods online and/or after others in their friend groups also announced transgender identities. She concluded that this appeared to be a novel type of presentation for which more research was needed.
Before even looking at Turban’s results, it is worth asking the question: is the YRBSS well-suited to examine any hypothesis related to ROGD? Does it contain data on: (1) sex; (2) transgender identification; (3) timing of onset of transgender identification with respect to puberty; (4) transgender identification of friends; and (5) type and duration of internet content prior to transgender identification?
The answers: (1) yes, but using language that may be ambiguous to trans-identified teens; (2) yes, but without separating out “non-binary” and other gender options, and only in about 15 states and a handful of school districts which chose to administer the question; (3) no; (4) no; and (5) no.
In order to confirm or refute the existence of ROGD, you would first need to make sure the data on which your study is based is capable of addressing the question at hand. Turban’s paper fails to clear even this first low hurdle.
Undeterred, Turban and colleagues assert that if the sex ratio of adolescents in the YRBSS does not favor females, which they claim it doesn’t, then this will count as evidence against the existence of ROGD as a phenomenon. But are they even correct in claiming that the sex ratio does not favor females? They state that the ratio of males to females in 2019 is, in fact, 1.2 to 1. Table 2 of their paper shows that this number is calculated as 1.7%/1.4%. The fascinating thing here is that Table 2 is clearly reporting raw data counts. There are no sampling weights and no acknowledgement of the complex survey design.
To see why this is important, let’s look at the distribution of responses across the included states. (Caveat: Turban and colleagues appear to have obtained Massachusetts data through a separate request, so those data are not included in the table below.) For 2019, here is how the data break down by unweighted and weighted frequencies for people who replied to the sex and the transgender identification questions:
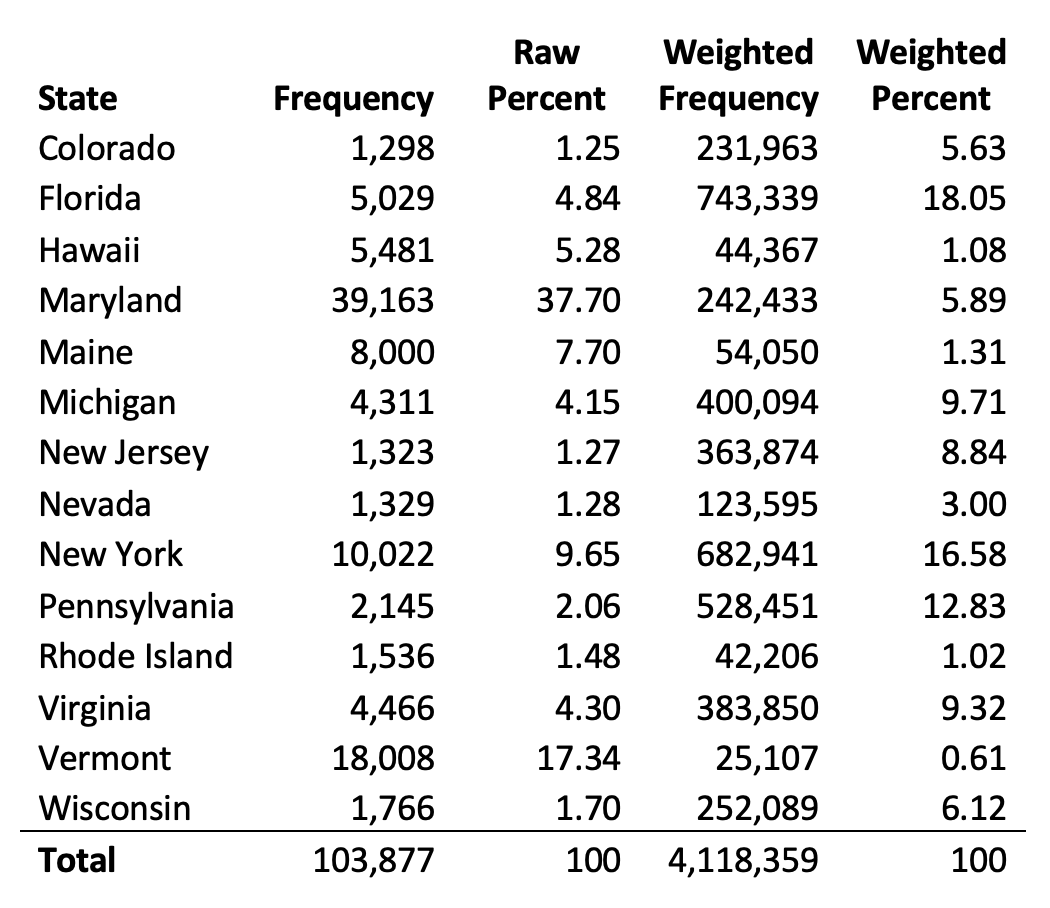
Using the weighted frequencies corrects for the fact that certain states are sampled far more heavily than others. By using raw data, Turban et al. have rendered their findings completely ungeneralizable, and indeed they seem to describe the small states of Maryland and Vermont more than any other. That being said, repeating the exercise using proper sampling weights yields rates of 1.54 percent for natal females and 1.67 percent for natal males. But because the standard errors overlap (a statistic not reported in Table 2), the finding here is that the rates of transgender-identification in the states that chose to administer the question in 2019 are roughly equal among natal males and natal females.
So, is Turban partly vindicated? To find out, we need to go back to the question of sex. In the paper, all individuals who leave “What is your sex?” blank were removed from the sample. However, transgender-identified teens are disproportionately likely to leave the question blank, and since we are dealing with very small numbers to begin with, even small sources of bias can lead to highly skewed results. Using sampling weights, 27.2 percent of those with missing data for sex were transgender, a rate that is 15 times higher than would be expected and is therefore clearly not random. If three quarters of these were natal females, this would be enough to create a sex ratio that (slightly) favors females. In other words, the missing data is not trivial. Moreover, while Turban et al. appear to believe that the “foundational salience” of sex will cause students to respond with their natal sex, many young trans-identified people routinely conflate “biological sex” and “gender identity,” so it is not at all a given that natal-female “trans guys” will mark themselves as “female” in the survey.
Taking a step back, what are the implications for ROGD if the sex-ratio in the population in 2019 is balanced between males and females? We know from several sets of gender clinic data that there have been sharp increases in total numbers presenting over the past decade, and that the sex ratios strongly favor natal females. We also have evidence from many of these clinics that the adolescents being referred typically have comorbidities that echo the findings of Littman’s paper. One obvious way to reconcile these findings is that the severity of the gender dysphoria involved, including mental health diagnoses and possible risk of self-harm, is a factor that may (1) motivate confused and trusting parents to bring a child to a gender clinic, or (2) motivate confused but skeptical parents to find like-minded parents on websites where Littman was able to recruit them into her study. The common denominator here is the degree of seriousness that parents may take regarding their child’s transgender declaration, which is likely to be correlated with the seriousness with which the child seems to take it.
Given that previous research on other social contagions, most recently including anorexia and behaviors mimicking Tourette’s syndrome, indicates that they disproportionately affect adolescent females, it is not unreasonable to assume young females may take their trans identities more seriously compared to males, resulting in heightened feelings of dysphoria.
Turban et al. also use the opportunity to note that rates of transgender identification actually dropped precipitously, rather than increased, between 2017 and 2019. By now you may be suspicious, and indeed, most of that finding disappears when sampling weights are used—and when the sample is extended to include all students who responded that they were transgender, regardless of whether they indicated their sex. The results below compare 2017 and 2019 for all respondents in states and districts that administered the question, with and without sample weights:

Indeed, within this geographic sample, there was a small decline between 2017 and 2019. However, there is significant overlap in the confidence intervals for the 2017 estimate (1.49 percent, 2.47 percent) and the 2019 estimate (1.29 percent, 2.23 percent), meaning there is no statistically significant difference in the rates of youth transgender identification between these years.
Let’s now turn briefly to the other finding, which relies on student reports of bullying to assess whether it is possible that some LGB young people prefer to identify as transgender “either to avoid sexual minority stigma or because being TGD will make them more popular with their peers.” Turban et al. find that rates of experiencing bullying (asked as “during the past 12 months, have you ever been bullied…?”) are most elevated among students who identify as trans. Perhaps relying on the “foundational salience” of sexual orientation, they take responses to these questions at face value. But what if our natal female “trans guy” prefers girls? Will she mark that she is “male” and “trans” and “heterosexual”? There is also a YRBSS question regarding the sex of sexual partners, and a cross-reference of that variable to the others shows that about 6 percent of students not identified as transgender state that they are gay or lesbian but have only had opposite-sex partners, whereas this was true for about 25 percent of trans-identified students. This strongly suggests the labels are being interpreted differently by different populations in the survey.
Regarding bullying, since the question was restricted to the previous 12 months, we lack information about the sequence of bullying and trans-identification. Turban et al. seem to be testing for a causal linkage, but to infer anything causal we would need to know the timing of bullying vs. timing of trans-identification. Otherwise it could just as easily be the case that a student began identifying as trans three months ago due to bullying that happened six months ago. Moreover, the variable does not assess frequency or duration of bullying, a factor that would seem relevant for understanding the degree of distress it might cause. Interestingly, there is another YRBSS variable that asks “during the past 12 months, have you ever been the victim of teasing or name calling because someone thought you were gay, lesbian, or bisexual?” It is unclear why the research team did not analyze this variable, which is much more specific to their research question.
While others have addressed some of the more obvious issues of Turban’s Pediatrics paper, the issues I’ve outlined above represent several more fundamental flaws that render the study incapable of empirically confirming or refuting the questions it purports to address.
Organizations to Support
 | A guest post by
|
Abigail Reed, excellent points! In addition, more points to consider:
1. The Trans Ideology considers "misgendering" to be bullying. Therefore, parents who are not affirming because it does not make sense are "bullying" as are siblings, as are old friends and grandparents. Needless to say, based on many, many videos, news shows, and now, Jon F-ing Stewart, families are debased and bullied.
I say he bullies me, as the ex-wife of a man who coerced me into staying, saying it was a mistake, then betrayed me with the help of his PhD "sexologist," by pretending he was on business trips when he was cross-dressing, for 2 and a half years, while I mothered our baby and toddler.
2. A study using N = all students who wrote answers in the blanks cannot be taken seriously. Students have not been oriented to a serious study, where you must say your natal sex for the sex question and must answer truthfully regarding your self-concept considering "gender." Gender is not defined.
3. Who funded the study, big pharma? Turban always, always uses "convenience samples" and there are no therapists, doctors, clinic staff or other trained adults recording what is happening. That would actually prove what we all know, the 4000% increase in suggestible teen girls saying they are really "boys." Or that category that means nothing, has no definition, "non-binary." Computer talk is the binary, synthetic thinking is non-binary, Turban fails in Logic, Biology, Genetics and Medicine. F-
“Dr. Lisa Littman ... coined the term “rapid-onset gender dysphoria” (ROGD) to describe a set of circumstances reported by parents participating in her study: adolescents who announced a transgender identity at or shortly after puberty after no childhood history of gender dysphoria.” No childhood history should be a big tell for anyone still wondering if this isn’t mostly social contagion. The dollars are there for this at scale if insurance companies are persuaded that these surgeries are necessary. Why else the Orwellian “gender affirming” to describe massive and irreversible changes to a child’s body. Changes he or she might regret as an adult.