

Suicide Mortality Among Gender-Dysphoric Adolescents and Young Adults in Finland
The finding of low suicide rates and no evidence of benefits of gender reassignment continues to challenge the practice of youth transitions.



Reality’s Last Stand is a reader-supported publication. Please consider becoming a paying subscriber or making a one-time or recurring donation to show your support.

This article was originally published on the Society for Evidence-Based Gender Medicine’s website on February 23, 2024.
A recent study published in BMJ Mental Health, “All-cause and suicide mortalities among adolescents and young adults who contacted specialised gender identity services in Finland in 1996–2019,” analyzed overall mortality and suicide mortality among gender-referred young people in Finland over a 25-year time span (n=2,083; median age 19 years; median follow-up 5.7 years). The study defined young people as those referred to gender services under the age of 23.
The study found that suicide among young people <23 (“youth”) seeking gender services in Finland is an unusual event (0.3%, or 0.51 per 1,000 person-years). Further, in comparing gender-referred youth to a cohort of matched controls (n=16,643), the study found no convincing evidence that gender-referred youth have statistically significantly higher suicide rates as compared to the general population, after controlling for psychiatric needs. The study also did not detect a statistically significant association between gender reassignment and the risk of suicide. The study did, however, find a statistically significant relationship between a high rate of co-occurring mental health difficulties and increased suicide. The authors concluded that “it is of utmost importance to identify and appropriately treat mental disorders in adolescents experiencing GD [gender dysphoria] to prevent suicide, while also noting that "the risk of suicide-related to transgender identity and/or GD per se may have been overestimated.”
This paper has important strengths and limitations. Its conclusions should be examined in the context of the preceding research from the Finnish team on the psychological needs of the recent cohort of youth presenting with gender dysphoria. An earlier study (also a registry study with no loss to follow-up), titled “Have the psychiatric needs of people seeking gender reassignment changed as their numbers increase?,” concluded that the level of psychopathology among gender-dysphoric youth has increased in recent years, but found no evidence that medical gender reassignment resolved psychiatric morbidity in young people experiencing gender-related distress.
In order to put the strengths and weaknesses of this latest research from Finland in context, we start by discussing the critical role the Finnish researchers played in highlighting problems with the practice of medical transition of adolescents. We then briefly expand on the most recent paper from the Finnish research team. We conclude with SEGM take-aways.
Background
Finland was the first country in the West to raise concerns about the practice of gender reassignment of minors. Finland opened its gender services for minors in January 2011, the same year as the first of two seminal Dutch papers—the paper focused on the outcomes of puberty blockers (de Vries et al., 2011)—was published. However, after the first few years of initiating youth gender transitions, Finnish clinicians began to sound the alarm. In their descriptively-titled 2015 paper, Two years of gender identity service for minors: overrepresentation of natal girls with severe problems in adolescent development, they observed that the majority of gender-dysphoric youth presenting for care were female, exhibited "severe psychopathology and considerable challenges in the adolescent development," and suffered from "wider identity confusion." The researchers cautioned that the concept of medical gender transition for this cohort was at odds with the principles of adolescent development.
In the majority of the applicants, gender dysphoria presented in the context of wider identity confusion, severe psychopathology and considerable challenges in the adolescent development. At this point it is not possible to predict how gender dysphoria in this group will develop: will gender dysphoria in these adolescents cease with the resolution of wider developmental problems, or perhaps consolidate later into transsexual identity, with the completion of the developmental tasks of adolescence.
The Finnish researchers continued to provide gender-transition services to youth, while continuing to note the increasing prevalence of gender-related distress in youth and the emerging role of social influence:
… GD appears more common than it was 5 years earlier among Finnish junior high school students. It remains to be seen whether this signifies a vastly increased need for SR services. Adolescents’ identity experiences are shaped by the surrounding society and extensive media coverage of topics related to transgender identity, GD, and gender reassignment, [which] may have an influence on how adolescents perceive themselves and their developmental distress.
By 2020, the Finnish researchers were in the position to evaluate treatment outcomes. While their 2020 paper is frequently quoted by proponents of youth gender transition as an illustration of success (during treatment with hormones, there was a reduction in visits related to depression, anxiety, suicidal ideation, and self-harm), the Finnish researchers themselves arrived at a much more nuanced conclusion with troubling implications. They reported that youth with significant mental health and functional problems at baseline not only failed to improve their functioning after they started hormones, but many got worse:
If the adolescents diagnosed with transsexualism had had difficulties at school/work as during the gender identity assessment, they mainly continued to have difficulties during the real-life phase. Only a minority moved from progressing with difficulties to progressing normatively, and equally many deteriorated during follow-up.
The focus on objective functioning—participation in school or employment, relationships with peers, romantic involvement, and gaining independence—were key outcome measures in the 2020 Finnish study. These measures of functioning are proxies for overall adolescent development. The Finnish researchers noted that gender transition does not appear to facilitate adolescent development in many gender-dysphoric youth, and indeed may exert a negative effect.
The data in the 2020 paper, along with a systematic review of evidence, led the Finnish Health Authority agency COHERE to issue updated recommendations for treating gender-dysphoric youth. These updated guidelines stipulated that psychosocial support and, if necessary, gender-explorative therapy was to be the first line of treatment, while hormone treatments were restricted to very few cases. In Finland, surgery was never allowed for youth under age 18.
While the Finnish research team published a number of other important research papers between 2015 and 2023, the two papers discussed above (Kaltiala-Heino et al., 2015 and Kaltiala et al., 2020) had arguably been the most groundbreaking papers from the Finnish gender research team—until this 2024 paper in the BMJ Mental Health.
Suicide Mortality in Gender-Dysphoric Youth: What Do We Know?
One of the strongest stated rationales for gender transition in youth is the aim to prevent suicides. The notion that suicides are common in gender-dysphoric youth, and that medical gender transition prevents this tragic outcome, is exemplified by the phrase “would you rather have a dead daughter or a living son?”
In February 2024, a new key paper, “All-cause and suicide mortalities among adolescents and young adults who contacted specialised gender identity services in Finland in 1996–2019” by the Finnish team was published in BMJ Mental Health. The paper posed three important questions (quoted directly from the paper below):
Do the all-cause and suicide mortalities of gender-referred adolescents differ from those of matched control populations?
Are any observed differences in mortality between gender-referred adolescents and matched controls explained by psychiatric morbidity?
What is the impact of GR [gender reassignment] on mortality among gender-referred adolescents?
In response to the first question specific to suicides, the researchers found that among <23-year-olds referred to the gender clinic between 1996 and 2019, 0.3% died by suicide, corresponding to 0.51 per 1,000 person-years. While this rate was about 4 times higher than the rate observed in the population of non-gender-dysphoric peers (0.12 per 1,000 person-years), the researchers found that once specialty psychiatric visits were controlled for, the difference between suicide rates in gender-referred adolescents and the general population was no longer statistically significant. In response to the second question, the study found that having 101+ psychiatric visits was a statistically significant predictor of suicide.
In response to the third question, the researchers were unable to find evidence that gender reassignment reduced suicide. When the gender-referred group was separated into “gender-reassigned (GR+)” and “not gender-reassigned (GR-),” and each group was compared to the general population (after controlling for the number of psychiatric visits as a proxy for psychiatric comorbidities), neither group's suicide rates differed from the general population in a statistically significant way. The researchers concluded that these results did “not support the claims that GR is necessary in order to prevent suicide.”
The paper has important strengths and limitations.
Strengths:
Objective and robust measure of suicide rates. The paper’s report of 0.51 per 1000 person-years, based on 13,602 person-years (with a median follow-up of about 6 years) represents one of the most robust measures of suicide in gender-dysphoric youth to date. Suicides should not be confused with “suicidality,” a related but distinctly different measure. Suicidality refers to a wide range of behaviors from thoughts about suicide and non-suicidal self-harm, to serious suicide attempts; it is usually assessed by self-report; it typically excludes actual suicides; and it is considered a less robust and reliable outcome. The large sample (over 2,000 cases of gender-referred youth) provides a high degree of confidence in the size of the estimate and strongly signals that suicide is an unusual event for gender-referred adolescents in Finland, regardless of their gender transition status.
Control for severe psychiatric comorbidities. Because psychiatric illness remains a key predictor of suicide, it is essential to isolate the extent to which gender dysphoria itself contributes to suicide risk in transgender-identified youth. The paper’s use of a proxy measure for severe psychiatric comorbidity allowed for a more reliable estimate of the effect of gender dysphoria on suicide (which was found to not be statistically significant). However, the chosen method of controlling for psychiatric comorbidities has important limitations, which we discuss below.
Isolated the effect of gender reassignment on suicides. One of the ongoing criticisms of the existing data on suicide is the inability to determine whether medical gender reassignment has a positive, negative, or neutral effect on suicides. This is because suicide is reported for gender-dysphoric patients without accounting for whether or not the patient was treated. The Finnish researchers controlled for treatment status by splitting the sample of gender-referred adolescents into “transitioned” vs “not transitioned” and comparing their suicide rates to the general population of matched peers. The paper concluded no effect of transition on suicides due to a lack of statistical significance. Our discussion in the "SEGM take-away" section below discusses the limitations of exclusively relying on statistical significance when too few events are observed, but we ultimately agree with the authors' conclusions.
No loss to follow-up. The paper used linked national health registries, which assured that all the assessed individuals were accounted for, with effectively no loss to follow-up (only those who left the country would be missing from the national register data). In contrast, most research in this field suffers from substantial loss to follow-up, ranging from 20% to 60%. Loss to follow-up can often mask negative outcomes, as patients disillusioned in their care or struggling with functioning are less likely to engage in follow-up research.
While this paper represents one of the most robust efforts to date to answer essential questions about the relationship between gender dysphoria and suicide, and the impact of gender transition on suicide, it also has important limitations. The most salient ones (some of which are recognized by the authors) are outlined below:
Limitations:
Relatively short-term follow-up. While the registry spans 25 years, the median follow-up time is under 6 years. Since the elevated morbidity and mortality in adult studies emerge after the 10-year mark, it is unlikely that the paper accurately reflects the long-term picture on adverse outcomes. Given the “honeymoon period” associated with gender transitions and the young age of current study participants, it is likely that the positive outcomes of the transition have been “frontloaded” and thus accounted for by the results, while the negative outcomes—including both the possibility of regret and the negative effect of prolonged exposure to cross-sex hormones—may not have been yet incurred and are not captured by the data. With longer follow-ups, the results could substantially change. However, this is a limitation of the field rather than the limitation of the study itself. Youth only began to present for gender reassessment in high numbers in recent years, which has contributed to the median follow-up of only about 6 years.
Too few events for a subgroup analysis. The welcome news that there were few suicides among the gender-dysphoric youth (n=7) comes with a scientific disadvantage that these numbers are too small for well-powered statistical analysis. For example, the study’s first two research questions led the researchers to compare 7 suicide events among gender-referred youth to 13 suicides in the matched control population. The analysis to inform questions about which independent variables (e.g., level of psychiatric comorbidity, transition status, sex, etc.) have an effect on suicide is necessarily limited by these small numbers. The small number of suicides is a welcome limitation.
Imperfect control for co-occurring mental illness. To assess the level of co-occurring psychiatric conditions, the researchers relied on the count of psychiatric visits to tertiary care. However, this approach does suffer from limitations. While the frequency of psychiatric visits is an indicator of severe psychiatric disease (the authors explain that in Finland, only severe psychiatric illness is treated at a tertiary level), it is an imprecise measure of psychiatric morbidity. For example, 1 psychiatric hospitalization, 1 outpatient consult for severe and persistent mental illness such as schizophrenia, and 1 visit related to depression would all count as "1 visit" but would signal different levels of psychiatric needs. At the same time, disorders such as anxiety may not be captured at all, if such less severe conditions are addressed at a lower level of care in the Finnish healthcare system. Further, while the researchers controlled for birth year, it does not appear that the number of psychiatric visits was annualized; instead, it was summed across the entire timespan. This risks underestimating the burden of psychiatric illness for most recently referred youth, who are presenting with large numbers in recent years with significant mental health comorbidities, but who have shorter psychiatric histories (fewer total visits).
The authors observe that “experiencing GD [gender dysphoria] significant enough to seek GR [gender reassignment] appears to not be associated with increased suicide mortality, but suicides appear to be explained by psychiatric morbidities.” They further note that:
When psychiatric treatment history is considered, GD significant enough to result in contact with specialized gender identity services during adolescence does not appear to be predictive of all-cause or suicide mortality. Psychiatric morbidities are also common in this population. Therefore, the risk of suicide-related to transgender identity and/or GD per se may have been overestimated.
Consistent with these observations, the authors finish with the clinical implication of the “utmost importance to identify and appropriately treat mental disorders in adolescents experiencing GD to prevent suicide” and recommended that “accurate information is provided to professionals” regarding this important topic.
The current study’s conclusions must also be examined in the context of earlier Finnish research. As mentioned above, another recent study from Finland, also relying on the registry data with no loss to follow-up, examined the psychiatric needs of gender-referred individuals in Finland. The study concluded that gender referrals at ever-younger ages are on the increase, with an increasing burden of co-occurring psychiatric problems. The authors examined the effects of gender transition on psychiatric needs, with the hope of seeing that gender reassignment, combined with reduced stigma and prejudice in society, would alleviate psychiatric comorbidities. Instead, the analysis showed that “manifold psychiatric needs persist regardless of medical GR [gender reassignment].” The authors noted that this conclusion from Finland is consistent with a recent US study, which also had no loss to follow-up.
SEGM Take-Away
The results of the study should be interpreted in the context of the unique characteristics of Finland's transgender-identifying population (e.g., the reportedly low rates of substance use in Finland, in contrast to the high reported rate in the US), Finland's recent strides in having significantly reduced suicide rates in the country overall, and Finland's unique, high-quality healthcare system, which contributes to superior health outcomes for the Finnish population. At the same time, several important aspects of the Finnish results are nonetheless likely generalizable to other Western countries, as the trend of high numbers of young people presenting to specialty services with a wish to medicalize their recent-onset transgender identity appears to be ubiquitous in the West.
The recent Finnish study confirms the earlier finding from the UK that suicides remain uncommon events in gender-dysphoric youth, regardless of gender transition status. It also confirms the finding from an earlier international study on suicidality (a related concept) that while the frequency of such events is elevated in gender-dysphoric young people compared with the general population of youth, it is comparable to youth referred for other mental health problems but not gender dysphoria. The Finnish study’s results suggest that the clinical management of gender-dysphoric young people should focus on the management of comorbid psychiatric conditions, which are a well-known risk factor for suicides. This conclusion is consistent with prior research, which consistently shows that psychiatric comorbidities are highly prevalent in gender-dysphoric youth, typically predating the diagnosis of gender dysphoria.
Some proponents of youth gender transitions may argue that while the effect of gender reassignment on suicide reported by the study was not statistically significant, it was nonetheless clinically meaningful. The study reported that youth who were gender-transitioned had a lower risk of suicide over time (adjusted hazard ratio, 0.8; 95% confidence interval 0.2 to 4.0; p-value = 0.8) compared to the general population, while youth who were gender-referred but did not undergo transition had a higher risk (adjusted hazard ratio, 3.2; 95% confidence interval 1.0 to 10.2; p-value, 0.05). Some have suggested that this signals that gender transition decreases suicide risk, and that this finding deserves careful consideration despite the lack of statistical significance, which could be explained by a small sample with insufficient power. In the past, SEGM itself made an argument that statistical significance alone should not be relied upon, and that some results can be not statistically significant, yet clinically meaningful.
Our analysis of suicidality data in the Bränström & Pachankis 2020 study is a case in point. Originally, the study concluded that hormones did not lead to improvement in mental health of gender-referred individuals but claimed that gender-affirming surgeries did result in a benefit. After the study’s publication, the analysis was found to have had significant problems, and the data were subsequently re-analyzed using a more rigorous statistical method. After the re-analysis, the earlier finding of benefits had to be corrected, stating, “the results demonstrated no advantage of surgery in relation to subsequent mood or anxiety disorder-related health care visits or prescriptions or hospitalizations following suicide attempts in that comparison.” In examining the re-analyzed data, SEGM noted that not only was the original conclusion of suicide attempt reductions nullified, but the re-analyzed data showed nearly twice as many serious suicide attempts in the “gender-dysphoric and surgically-transitioned” group relative to the risk-matched “gender-dysphoric but not surgically-transitioned” group. While this difference was not statistically significant, we argued that it was nonetheless clinically meaningful, and that the lack of statistical significance was likely due to lack of power from too few recorded suicide attempts.
For the reasons outlined above, we will engage with the question, does the Finnish data show that gender transition reduces suicides—even if the results were not statistically significant?
Does the Finnish Study Show That Gender Transition Reduces Suicides?
Statistical significance is a double-edged sword. On the one hand, statistical significance testing is an objective method that separates the “signal” from the “noise” of random error in a dataset, so that random effects are not mistaken for a likely true effect (also known as Type I error). On the other hand, it is possible to wrongly dismiss a real effect because it failed to reach statistical significance, for example, due to a small sample (known as Type II error). For this reason, besides looking at statistical significance, one should examine the direction, magnitude, and precision of effect estimates (i.e., confidence intervals), as well as the overall sample size. It is possible to come to a conclusion that a non-statistically significant result is still clinically meaningful and informative.
Below we explain why the Finnish results do not suggest that gender transition reduced suicides. In fact, had the results been statistically significant, we would still assert that one could not draw the conclusion that Finnish data provided reliable evidence that gender transitions reduced suicides. This is because we believe the adjustment for psychiatric illness, which is one of the strongest predictors of suicide, did not fully account for the burden of psychiatric comorbidity, and that this limitation disproportionately affected the “gender-referred but not reassigned” (GR-) group’s comparison to the general population, leading to a possible overestimate of the point estimate for the adjusted hazard ratio.
Because the researchers chose to rely on the total count of psychiatric visits to specialty tertiary care centers as their control variable, the analysis remained vulnerable to confounding due to psychiatric illness, as we explained in the limitation section above. This limitation is particularly relevant to the discussion at hand because the assignment to “gender-referred but not reassigned” (GR-) vs. “gender-referred and reassigned” (GR+) groups was non-random. Individuals with a higher degree of psychiatric comorbidity, and, thus, a higher baseline suicide risk, were less likely to be approved for transition by the centralized Gender Identity Services (GIS), and, thus, more likely to “end up” in the GR- group, as the quote from the earlier 2023 Finnish study suggests:
Proceeding to medical GR [gender reassignment] interventions was not independent of psychiatric treatment needs prior to contacting GIS. Those who proceeded to medical GR presented less commonly with needs for specialist-level psychiatric treatment before contacting GIS and after the index date.
Given the well-established fact that recent gender-referred youths suffer from high rates of co-occurring mental illness, the inability to fully control for psychiatric comorbidity would likely disproportionately affect the GR-group's comparison to the general population, affecting the adjusted hazard ratios calculations.
Of course, the lack of statistical significance is another strong reason not to over-interpret the difference in the point estimates in the adjusted hazard ratios between the GR+ and the GR- groups. The confidence intervals for adjusted hazard ratios for suicide between GR- and GR+ (compared to controls) were 1.0 - 10.2 and 0.2 - 4.0, respectively. In other words, among gender-referred young people who underwent medical reassignment (GR+), the rate of suicide was anywhere from 80% lower to 4 times higher than matched controls, after accounting for psychiatric comorbidity, whereas among gender-referred young people who did not undergo medical reassignment (GR-), the rate of suicide was the same as or up to 10 times higher than matched controls. The uncertainty around the estimates was due to the (thankfully) small number of suicides in both groups.
Perhaps most importantly, debating whether these non-statistically significant study results can still be interpreted to mean that gender reassignment reduced suicides misses the biggest point of the study: the low absolute risk of suicide in the population of gender dysphoric youth. Because this absolute base risk is low, any further treatment-associated reductions in the risk are naturally limited and must be considered in the context of the harms of the same treatment, as we explain below. (To clarify, the explanation below is based on a thought experiment, as the researchers did not share the raw numbers due to patient privacy reasons.)
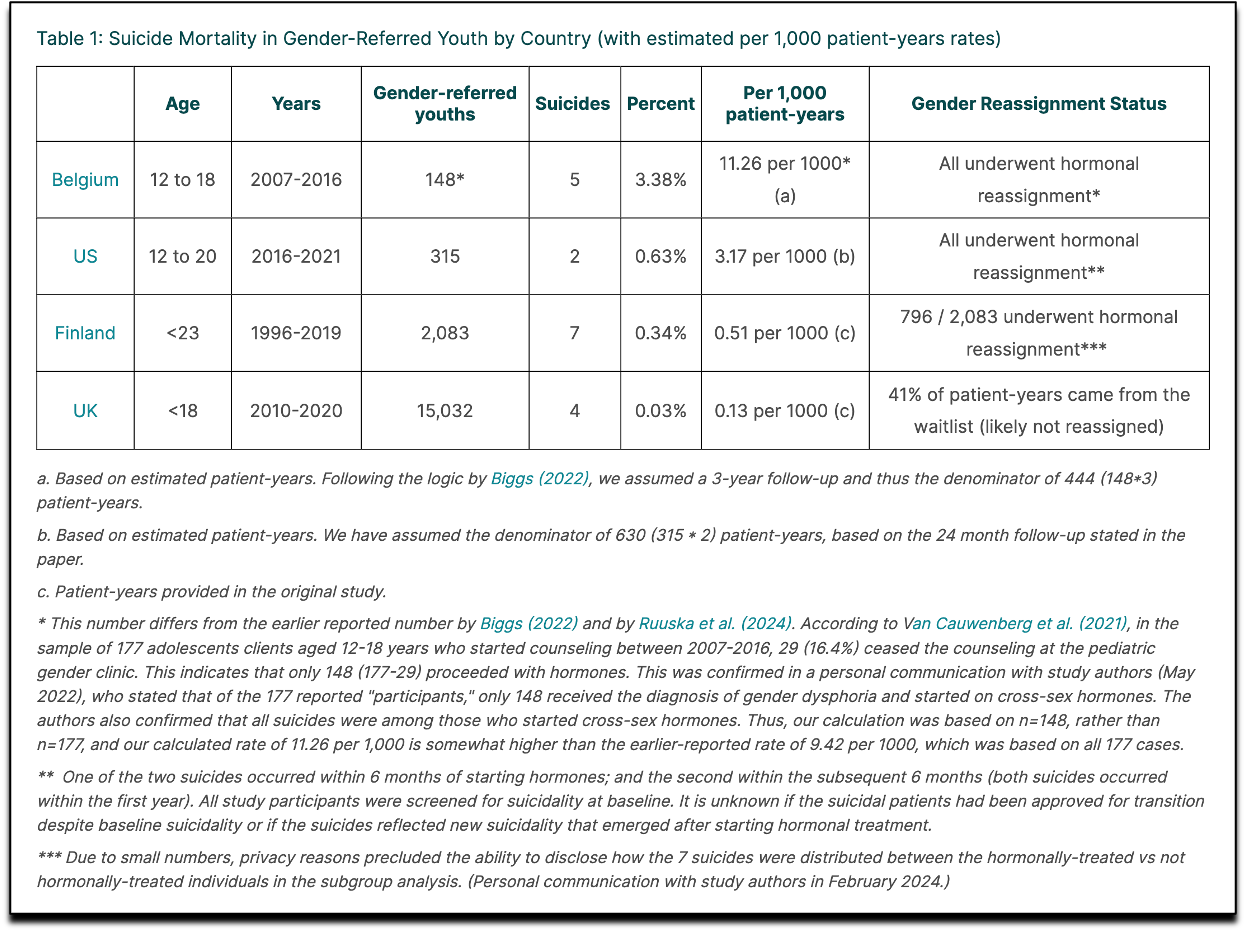
Let’s assume that 6 of the 7 recorded suicides in the Finnish study occurred in the GR- (un-reassigned) group (6/1287=0.47%), and only 1 of the 7 suicides occurred in the GR+ (reassigned) group (1/796=0.13%); this is the most generous assumption the current data affords. Although one could claim that suicides were reduced nearly 4-fold (from 0.47% to 0.13%), the absolute suicide risk was reduced by less than 1 percentage point (0.47%-0.13%=0.34%). This example emphasizes the need to always consider the absolute, rather than relative risk. Reliance on relative risk reduction can lead to an overly optimistic (and often misleading) assessment of a treatment's efficacy.
Further, any reductions in the risk of suicide from gender reassignment, which are limited by the ceiling of less than 1% as we demonstrate above, must then be weighed against the risk of treatment-associated harms. For example, every child treated according to the recommendations by the Endocrine Society (i.e., starting puberty blockade at Tanner stage 2 and followed with cross-sex hormones) is expected to be infertile or sterile, and significant unanswered questions remain about bone and brain development. Past studies of transgender-identified adults found significantly shortened lifespans and elevated morbidity among transitioned individuals, including significant cardiovascular risks. A number of other risks emerge saliently only after the 10-year mark, which is several years later than the study's average follow-up of 6 years. While the Number Needed to Treat (NNT) to avoid an adverse outcome such as suicide is impossible to calculate from the current study, given the hypothetical best-case-scenario example above, the relationship between the NNT (number needed to treat) and the NNR (number needed to harm) is unlikely to be favorable, even if gender transitions did reduce suicides—which the study failed to conclude.
Finally, trading off benefits and harm involves patient and parent (in the case of minors) value judgments about how much harm (and what type) a patient would accept in return for a benefit. Quality systematic research into patient values and preferences in this space has not been conducted.
In constructing Table 1 below to summarize what's known about the absolute risk of suicide in gender-referred youth, we noted that the highest rates of suicides were reported in instances where every young person was treated with hormones. That neither the current study nor several other studies to date have been able to demonstrate that gender transition reduces suicide or serious suicide attempts adds to the concern that the suicide narrative has been inappropriately used to promote medical gender transitions of youth.
We would like to conclude our discussion of the Finnish study with a recent quote from Dr. Erica Anderson, the former President of USPATH: “If gender-affirming medicines could not provide sufficient relief to the adolescents so treated and reduce their suicidality, should such patients have received hormones at all?”
We would like to add one more important question: How should the treatment outcomes be measured? The medical community must come to a consensus on what the primary treatment target is. The goal of suicide reduction, which has long been asserted by the many proponents of youth gender transitions, appears to be a flawed measure. At the same time, a mere achievement of satisfying appearance results, as suggested by the new “gender incongruence” ICD diagnosis, is also a questionable measure, especially given what we know about ongoing adolescent development.The Finnish researchers have long asserted the treatment target should be on the improvements in functioning (both short- and long-term).
These critical questions must be urgently debated by the professionals who deeply care about helping gender-dysphoric youth. The answer to these questions will have a direct impact on which treatments—hormones and surgery, or watchful waiting and psychotherapy—will become the standard of care for the rapidly growing numbers of gender-dysphoric youth in the 21st century.

Reality’s Last Stand is 100% reader-supported. If you enjoyed this article, please consider upgrading to a paid subscription or making a recurring or one-time donation below. Your support is greatly appreciated.

Bibliography
The bibliography of the Finnish research, including the four latest papers, is below, arranged by the year in reverse-chronological order
Ruuska, S.-M., Tuisku, K., Holttinen, T., & Kaltiala, R. (2024). All-cause and suicide mortalities among adolescents and young adults who contacted specialised gender identity services in Finland in 1996–2019: A register study. BMJ Mental Health, 27(1), e300940. https://doi.org/10.1136/bmjment-2023-300940
Kaltiala, R., Holttinen, T., & Tuisku, K. (2023). Have the psychiatric needs of people seeking gender reassignment changed as their numbers increase? A register study in Finland. European Psychiatry, 66(1), e93. https://doi.org/10.1192/j.eurpsy.2023.2471
Ruuska, S.-M., Tuisku, K., & KalGala, R. (2023). Hormonal and surgical treatment for gender dysphoria in young people – beneficial or not? [Sukupuoliahdistuksen hormonaalinen ja kirurginen hoito nuoruusiässä – hyötyä vai ei?]. Suom Lääkäril [Finnish Medical Journal], 78(43–44), 1760–1763. https://www.laakarilehti.fi/site/assets/files/654775/article_pdf_73878.pdf
Kaltiala, R., & Karvonen, M. (2023). Sukupuoliahdistus, transgender-identiteetti ja mielenterveys nuoruusiässä [Gender dysphoria, transgender identity and mental health in adolescence]. Duodecim, 139, 487–493. https://www.duodecimlehti.fi/duo17611
Karvonen, M., Karukivi, M., Kronström, K., & Kaltiala, R. (2022). The nature of co-morbid psychopathology in adolescents with gender dysphoria. Psychiatry Research, 114896. https://doi.org/10.1016/j.psychres.2022.114896
Kaltiala, R., Bergman, H., Carmichael, P., de Graaf, N. M., Egebjerg Rischel, K., Frisén, L., Schorkopf, M., Suomalainen, L., & Waehre, A. (2020). Time trends in referrals to child and adolescent gender identity services: A study in four Nordic countries and in the UK. Nordic Journal of Psychiatry, 74(1), 40–44. https://doi.org/10.1080/08039488.2019.1667429
Kaltiala, R., Heino, E., Työläjärvi, M., & Suomalainen, L. (2020). Adolescent development and psychosocial functioning after starting cross-sex hormones for gender dysphoria. Nordic Journal of Psychiatry, 74(3), 213–219. https://doi.org/10.1080/08039488.2019.1691260
Kaltiala-Heino, R., & Lindberg, N. (2019). Gender identities in adolescent population: Methodological issues and prevalence across age groups. European Psychiatry, 55, 61–66. https://doi.org/10.1016/j.eurpsy.2018.09.003
Kaltiala-Heino, R., Työläjärvi, M., & Lindberg, N. (2019). Gender dysphoria in adolescent population: A 5-year replication study. Clinical Child Psychology and Psychiatry, 24(2), 379–387. https://doi.org/10.1177/1359104519838593
Kaltiala-Heino, R., Bergman, H., Työläjärvi, M., & Frisen, L. (2018). Gender dysphoria in adolescence: Current perspectives. Adolescent Health, Medicine and Therapeutics, Volume 9, 31–41. https://doi.org/10.2147/AHMT.S135432
Kaltiala-Heino, R., Sumia, M., Työläjärvi, M., & Lindberg, N. (2015). Two years of gender identity service for minors: Overrepresentation of natal girls with severe problems in adolescent development. Child and Adolescent Psychiatry and Mental Health, 9(1), 9. https://doi.org/10.1186/s13034-015-0042-y
 | A guest post by
|
Brilliant . Yet the medical community is pushing this propaganda on children . All about money . Sickening.
If one’s response to opposition is to contemplate suicide, rather than to attempt to circumvent the opposition, it would seem this is in itself evidence of psychopathology.