

Britain’s Study of Puberty Blockers Will Mostly Be a Pointless Waste
The study’s leaders have announced it will proceed after all. But absent a planned 2nd phase to study cross-sex hormones, the trial is likely to amount to not much more than a $14 million cash sink.



Reality’s Last Stand is a reader-supported publication. Please consider becoming a paying subscriber or making a one-time or recurring donation to show your support.

About the Author
Benjamin Ryan is an independent journalist, specializing in science and health care coverage. He is a contributor for The New York Times, The Guardian, NBC News, The Free Press, and The New York Sun. He has also written for the Washington Post, The Atlantic and The Nation, among many others. Follow him on X: @benryanwriter. Visit his website: benryan.net
This article was originally published on the author’s Substack: Hazard Ratio.
King’s College London on Friday announced that, after a period of reflection and regrouping amid outcry from all sides, the leaders of the much-debated, much-ballyhooed National Health Service clinical trial of puberty blockers for gender-distressed youths would continue largely as planned.
The study’s design has received just a few tweaks, most notably the addition of new minimum ages for participants: 11 years old for natal girls and age 12 for natal boys.
Otherwise, it’s full steam ahead for the £10 million, or $14 million, study.
But anyone who understands even the basic parameters of how pediatric gender medicine works—and what the central purpose of this medical field is—can see that this clinical trial, which if designed properly might have afforded the world some desperately needed insights into these controversial medical practices, is headed straight into the scientific abyss.
Multiple observational studies, including one conducted by the NHS itself and published in 2021 and another, long-delayed study out of the United States that finally emerged in preprint last year, have already found that minors who take puberty blockers to treat gender dysphoria or gender incongruence see essentially no change in major mental health metrics. Such disappointing conclusions stood in contrast to the more glowing findings of the foundational cohort study out of the Netherlands that was published in 2011 and helped spark global excitement and launch the pediatric gender medicine field worldwide.
The authors of the U.S. puberty-blocker study, led by Dr. Johanna Olson-Kennedy, formerly of Children’s Hospital Los Angeles, rationalized the lack of apparent benefit from taking puberty blockers by suggesting that the mental health of youths on these drugs would have worsened absent the medication.
That may very well be true, and such a premise points to the fact that these medications have only ever been meant to tee up treatment with cross-sex hormones. A coterie of pediatric gender medicine advocates, in fact, wrote an amicus brief for last year’s U.S. Supreme Court case over Tennessee’s ban of gender-transition treatments for minors in which they criticized Britain’s Cass Review for conceiving of blockers and hormones as anything but part and parcel of one another.
The fact is that almost all youth who take blockers for gender dysphoria go on to take hormones, according to multiple studies, including at the NHS. As British journalist Hannah Barnes wrote in her seminal investigation of the NHS’s doomed pediatric gender clinic, Time to Think, it is essentially unheard of in psychology to have any sort of test that has a close-to-perfect accuracy rate. In other words, gender-clinic providers haven’t simply succeeded brilliantly at selecting all the right kids to put on this treatment pathway, especially given how cursory, rushed or non-existent the assessment process can be at these clinics.
Considering all this, it is abundantly evident that gender-dysphoric adolescents have never conceived of the period they must spend on blockers as a “time to think” about their gender, as leaders in pediatric gender medicine long misled the public to believe (that is, before at least some of them conducted an about-face and started insisting, accurately, that blockers and hormones are simply part of a continuum). These youths quite clearly view the blockers as a waystation, a temporary burden they must satisfy on behalf of adult authority figures before they get what they actually want: hormones.
Given the planned NHS study, called PATHWAYS, has a randomized element—youths will be randomly assigned to go on blockers immediately or following a one-year delay—there was at least some hope that the study could have produced higher quality evidence than the critically flawed collection of studies that have been produced to date.
None of the past or ongoing studies of gender-transition treatment for youths have been randomized controlled trials. Instead, they are largely a messy and compromised collection of prospective cohort studies that for the most part have no comparison groups and typically have short follow-up times of 12 to 24 months. Or, in the case of Kristina Olson’s study out of Princeton, there is an ever-lengthening follow-up time, but the cohort is not at all representative of the typical youths presenting at a gender clinic these days, given the participants typically socially transitioned very young, by age six or seven.
So the whole world has turned its eyes Britain in hopes that, being an island nation that in 2024 passed a strict legislative ban of puberty blockers for minors outside of a clinical trial, the NHS might manage to recruit and retain a sizeable population of youths seeking gender-transition drugs. Denied other (legal) means of obtaining these drugs (hormones are blocked for those under 16 and are increasingly hard to get even for older minors in the UK), British youths might stay in the study even if they aren’t randomized to receive blockers immediately.
But if youths in PATHWAYS aren’t provided hormones after starting blockers, it is highly likely that all we will learn from this lengthy and expensive clinical trial—youths are set to receive blockers for up to two years and the study is slated to run for five-and-a-half years overall—is more of what we already know: that not much happens psychologically when these kids take blockers.
Furthermore, there isn’t much puberty actually to arrest among the youths who present at gender clinics these days. Recent research out of the United States, including one analysis of national insurance data and a comparable analysis focusing on Oregon, have suggested that only a fraction of the minors who receive gender-transition interventions actually take puberty blockers. And an even smaller minority start such treatment when they are young enough to be in puberty’s early stages.
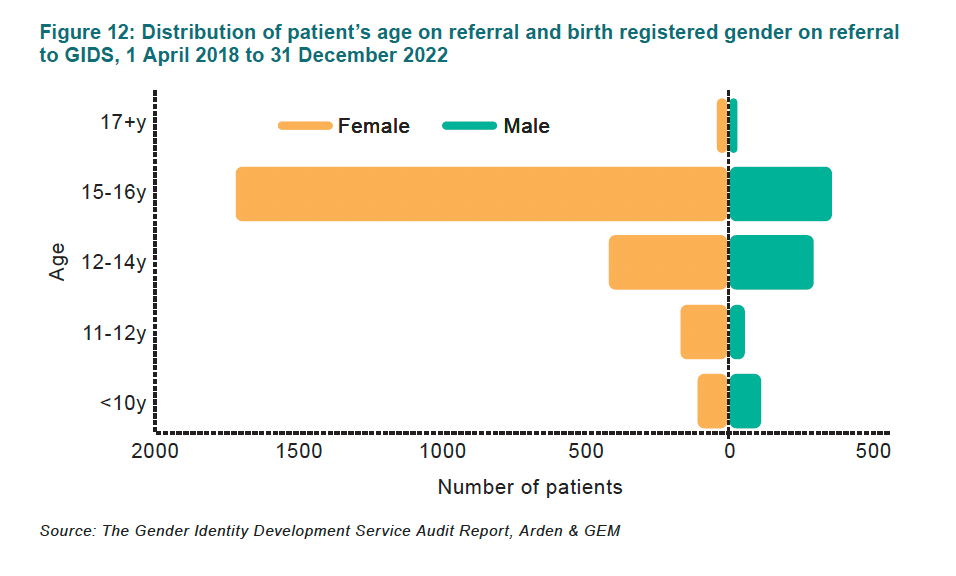
The typical youth who presents at a gender clinic in the Western world these days, including in England, is a 14- to 16- year-old biological girl who only began exhibiting gender-related distress after puberty’s onset. PATHWAYS will only accept youths who are under age 16 when entering the study. So, given the age and sex breakdowns of youths upon their referrals to Britain’s since-shuttered gender clinic (see the chart below, from the 2024 Cass Review), that means that the bulk of the youths eligible for this new study will likely be 14- and 15-year-old natal girls.
Such youths are likely either in the final phase of puberty or are entirely finished with the developmental process. PATHWAYS, per its inclusion criteria, welcomes youths who are in any of the so-called Tanner stages of puberty, from Tanner 2 (the earliest phase) to Tanner 5 (meaning puberty is finished). So by the study authors’ own admission, they are perfectly willing to give puberty blockers to minors with no puberty to block.
Given that natal females have no physiological need to take blockers in advance of starting testosterone (for natal males, blockers can help suppress their natural testosterone production and thus supplement estrogen treatment), for these youths, starting blockers amounts to all risks with no clinical purpose.
Representatives for King’s College London, which is leading the trial on behalf of the NHS, did not respond to my brutally frank request for comment. Otherwise, in their press release announcing the slight revisions to the trial, they stated: “We will always welcome scrutiny of research involving children and young people because their health and safety is paramount. Our priority remains to safely, and robustly, investigate the benefits and risks of puberty suppression for young people with gender incongruence to improve the evidence base and inform NHS healthcare.”
The PATHWAYS study does have an important element in which some of the youths will receive a series of brain scans. This is perhaps the only part of the overall research endeavor that could yield vital results that could help inform worldwide care of gender-dysphoric youths. According to a 2024 review paper, scientific knowledge of the impacts of puberty blockers on the brain remains woefully thin. And there are concerns that the powerful drugs might have deleterious impacts on neurocognition.
Blockers are supposed to be the warm-up act to the main event, in which, at least in theory, people who identify as transgender spend a lifetime on cross-sex hormones—or, in the case of natal females in particular, they stay on testosterone long enough to permanently deepen the voice and prompt the permanent growth of facial and body hair.
Considering all this, why in heaven’s name isn’t the NHS planning to study cross-sex hormones in youths?
Is this study simply an expensive charade to kick the political can down the road?
This article was originally published on the author’s Substack: Hazard Ratio.
If you enjoyed this free article, please consider upgrading to a paid subscription or making a recurring or one-time donation below to show your support. Reality’s Last Stand is a reader-supported publication, and your help is greatly appreciated.
If you enjoyed this article, you may also like…




 | A guest post by
|
The cult behind all of this will never recognize rational thinking and scientific principles. The advocates promoting younger and younger children in ideations and delusions will not admit that no one can make these decisions with informed consent. By this I mean adults as well as children. I just saw a young adult male, clearly male from his 6 ft height, the size of his large hands, head, the hip/shoulder ratio, etc, picking up estrogen and some kind of testosterone blocker. How do I know what he got from the pharmacist? He asked in a rather loud voice whether the estrogen was through injection. Why was he talking so loudly? Because he had his entire lower facial area covered with a black mask. He also appeared to be borderline anorexic. Don't be one of the "nice" people who will use female pronouns for this psychiatrically ill male patient, as it is like telling an anorexic they'll look even better if they just drop 5 more pounds.
A question here. In the M2F case it is my understanding that simply blocking testosterone in early adolescence will result in the individual developing a rather female body pattern, rather than a distinctive masculine pattern. The later addition of estrogen++ would complete the feminization, but even without the additional hormones the individual is likely present as rather feminine, just on a slower time scale than they would have with active hormone treatment.
Am I correct?